Saturday, March 28, 2020
A Few Thoughts on COVID-19 - Part II
One week ago, I wrote:
As of today, the global COVID-19 fatality rate (deaths divided by aggregate confirmed infections) is about 4.1%.
We know that the actual fatality rate is probably significantly lower than 4.1% because not everyone who has been infected has been tested.
There are a lot of other factors leading to uncertainty over the actual fatality rate from COVID-19 that I didn't write about. There is an excellent discussion of the "Coronavirus (COVID-19) Mortality Rate" that elaborates on those factors. I recommend it.
Today, the crude global COVID-19 fatality is about 4.6% per figures from the UW Novel Coronavirus (COVID-19) Infection Map. I still have every expectation that the final rate will be much lower than 4.6% globally, in Italy, the US, and elsewhere. However, because of the failures mentioned in my earlier post I still fear that "the progression of the COVID-19 in the US will likely resemble Italy's trajectory more closely than South Korea's or China's." Nothing that's happened in the last week has dissuaded me from that view although I remain hopeful something will change.
A week ago, I also wrote: "By the end of next week we may start to see how effective efforts to flatten the curve have been in Washington state." The Governor of Washington believes this may be the case but in my reading of the data it's still too soon to know for sure.
I want to elaborate a bit on the comparison I made between the US and South Korea. China, in my opinion, is the wrong place to look for comparisons. Although China has some aspects of a market economy, large and important entities are state-owned enterprises directly controlled by the Communist Party of China (CPC) and the remaining sectors are subject to indirect CPC control in the one-party authoritarian regime.
There is evidence that the Chinese government suppressed key information about the virus at least in the early stages. In contrast, South Korea has a modern, mostly private market economy with a political system that is, by one measure, at least as democratic as the United States' "flawed democracy" (but see here for a different ranking).
One of the big mistakes that many people will undoubtedly make in the aftermath of COVID-19 is to demand a larger, more centralized public health and medical system in the US. One of the big pitfalls of such thinking is that centralization creates the risk of severe consequences from a single point of failure.
We are actually seeing that play out in the US where state and local public health agencies and officials take their lead from the federal government and were slow to react appropriately to the threat of COVID-19. They were also hamstrung by their dependence on the Centers for Disease Control and Prevention (CDC) to roll out COVID-19 testing and misplaced reliance on supplies from the Strategic National Stockpile (SNS).
One counterargument is, yes, but if the federal government had done its job correctly then we wouldn't be in this situation. True enough but there are no guarantees that when a crisis develops there will be an able, humane leader at the helm of the large, centralized ship of state.
I am aware of no compelling evidence that, say a President Hillary Clinton, would have prepared for or handled the COVID-19 crisis markedly better than Trump. Speculatively, we can say she may indeed have risen to the challenge of COVID-19 but Clinton would have been under the same pressures by the investor class not to disrupt their profit-taking and to win re-election this year.
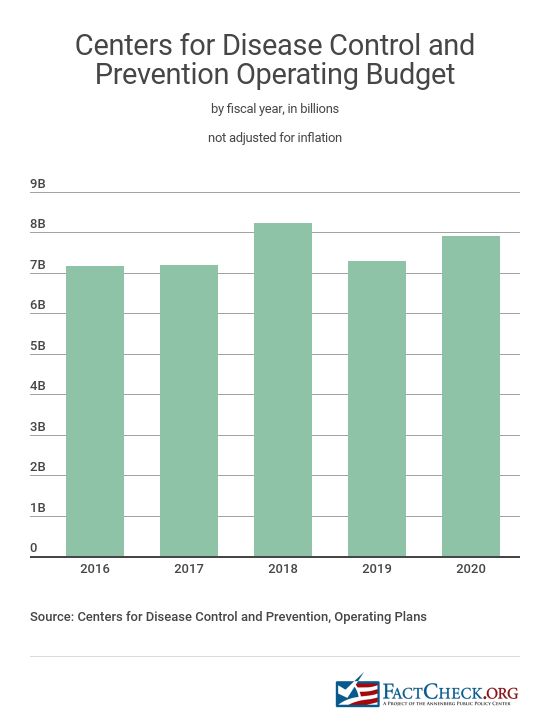
More crucially, the lapses in the CDC and the SNS, for instance, didn't develop under Trump alone. I have been unable to find a concise depiction of inflation-adjusted CDC annual budgets (there is this though) but it's clear that the Obama administration proposed significant cuts in 2011 (-11%). In 2013, the Obama administration again proposed more cuts in "biodefense and emergency preparedness programs" along with a $38 million reduction in the "allocation for the Strategic National Stockpile of emergency medical supplies".
And as NBC reports:
[The] U.S. strategic stockpile isn't intended to be the solution to a crisis. It's designed to be used as a stopgap during emergencies. The stockpile has limited resources, government officials and public health experts say, which weren't at full capacity even before the coronavirus was on the horizon.And:
The stockpile wasn't at full capacity before the COVID-19 outbreak in the U.S., in part because it never fully replenished some of the critical supplies used in the 2009 H1N1 pandemic response ...A 2016 report published by the National Academies repeatedly raised concerns about the SNS inventory and the logistics of distributing it in an emergency. The chair of the committee that prepared that report, Dr. Tara O'Toole, presciently told NPR in 2016:
"We have drastically decreased the level of state public health resources in the last decade. We've lost 50,000 state and local health officials. That's a huge hit," says O'Toole, who wishes local officials would get more money for things like emergency drills. "The notion that this is all going to be top down, that the feds are in charge and the feds will deliver, is wrong."My point is that the inability and failure in the US to implement the successful model of South Korea to tamp down COVID-19 via widespread testing, contact tracing, and isolation of the exposed or infected was born of a longstanding failure of the values and priorities of the bipartisan political establishment and by the servile dependency and doltish complacency of the American people who keep electing them. Trump surely deserves a lot of blame for his failures but much of the finger pointing by, for example, Michigan Gov. Whitmer, is simply not grounded in fact and is counter-productive, self-interested blame-shifting by culpable partisans in the midst of a major crisis.
It bears stating that governments weren't invented for the well-being of commoners and only servile fools would willingly depend upon them for that. Governments were created to secure and enhance the power of the already powerful and to provide rhetorical cover for that domination. That is not to say they cannot potentially be transformed by people to more closely reflect the rhetoric of, say, "life, liberty, and the pursuit of happiness" but we should never forget that decent treatment of ordinary people is, at best, a means, not an end, of government.
If we are to have a centralized state or any state at all then, ceteris paribus, one that could competently stop an COVID-19 epidemic, for instance, would be preferable but this is a false dichotomy. There are other, better ways for humans to organize themselves free from the coercive state if only we will imagine and create them.
See also: "A Few Thoughts on COVID-19"
Labels: anarchism, COVID-19, government, health, medicine, politics, science, Trump
Saturday, March 21, 2020
A Few Thoughts on COVID-19
Don't be deceived, COVID-19 is more lethal and more infectious than the normal annual influenza outbreaks. As one example, in roughly three weeks COVID-19 has already killed almost as many people in the Seattle area (King, Snohomish, and Pierce counties) alone as have died so far from the flu (lab-confirmed cases) in the entire State of Washington during the 2019-2020 flu season and COVID-19 shows no sign of slowing down yet. In part, this is because almost no one has any natural or vaccine-induced immunity to COVID-19 as it is "novel" and there is no vaccine for it.
Everywhere that COVID-19 has infected large numbers of people it has quickly overwhelmed the local health care system. That means the death toll from COVID-19 is added on to the existing, more routine causes of death from heart disease, cancer, influenza, accidents, etc. and the rapid influx of those sick from this new disease impairs the health care system's capacity to manage more typical cases of disease and trauma.
If unchecked by effective public health measures or natural immunity COVID-19 has exponential growth rates of infection and death (see also here and here and here) although the death curve is much flatter because the disease does not kill at nearly the same rate as it infects or sickens people. As of today, the global COVID-19 fatality rate (deaths divided by aggregate confirmed infections) is about 4.1%.
We know that the actual fatality rate is probably significantly lower than 4.1% because not everyone who has been infected has been tested. In South Korea, where there are high rates of testing and a very successful public health response, the fatality rate is about 1.2%. By contrast, the US 2018-2019 influenza fatality rate was about 0.1%. (There are a lot of factors, such as quality of the health care system, mean population age, smoking rates, etc., that influence fatality rates.)
Below, from the University of Washingon Novel Coronavirus (COVID-19) Infection Map, are two images (click to enlarge) showing the exponential growth of COVID-19 infections and deaths in the US and Italy.


The graphic below demonstrates that exponential growth of infection and death from COVID-19 can be arrested. South Korea had its first confirmed COVID-19 death on February 21 and in about three weeks it had stopped the initial exponential growth of infections. The number of COVID-19 deaths there is currently 102. China, too, after early missteps has reportedly stopped local transmission of COVID-19 altogether.

We did have earlier warnings to alert us to the potential of a dangerous viral pandemic. In addition to the Spanish Flu (1918; 25,000,000 - 100,000,000 deaths), there was the Asian flu (1957; 1,000,000 - 2,000,000 deaths), Hong Kong flu (1968; 1,000,000 - 4,000,000 deaths), SARS-CoV (2002; 774 deaths), H1N1 flu (2009; 151,000 - 575,000 deaths), and MERS-CoV (2012; 862 - 912 deaths). MERS is notable because it has a high fatality rate (~37%) and continues to infect and kill people every year. With few exceptions, the media, public health community, and politicians of all political stripes failed to alert Americans to the very real dangers of a viral pandemic and the country is, thus, woefully unprepared.
Unfortunately, I am afraid the progression of the COVID-19 in the US will likely resemble Italy's trajectory more closely than South Korea's or China's. I hope I will be proven mistaken in this.
American individualism is, in many ways, pathological and more communal attitudes and behavior are not necessarily antithetical to freedom or a healthy individualism. Whatever their downside, a more community-oriented culture was one factor that evidently contributed to the successful Chinese and South Korean responses to COVID-19.
If competently led, adequately staffed, and sufficiently provisioned, I think America's decentralized health care system could have responded in a coordinated and effective manner. This was not the case, however, and one result has been the very slow roll out of widespread COVID-19 testing that would have enabled the early isolation of infected people. The US also has a warped, hollowed out industrial base that has left it dependent on the importation of key health care supplies—masks, drugs, reagents, gloves, ventilators, etc.—that were seemingly not stockpiled and/or aren't being distributed in sufficient quantities.
Chinese health officials were able to successfully confine the COVID-19 outbreak to primarily one region of the country and then bring the resources of the rest of the country to bear in order to tamp down the disease. Unfortunately, for reasons described above, the US has failed to keep the outbreak of disease concentrated in one or two regions.
The result is that the COVID-19 is now, apparently, spreading exponentially in every US state. The first US death from COVID-19 was on February 29, 2020. Since that time Washington has had 82 more deaths, New York 43, California 24, Louisiana and Georgia 14 each, New Jersey 11, and Florida 10. COVID-19 deaths have been reported in several other states, too. The wide geographic dispersion of infections in the US will likely make it immensely difficult to bring COVID-19 under control quickly. Again, I hope I am proven wrong in this.
By the end of next week we may start to see how effective efforts to flatten the curve have been in Washington state. However, even if they have been effective the state has already fallen far short in comparison to South Korea. Consider the table below based on the 2018 populations.
| COVID-19 Deaths Per 100,000 Population | Days Elapsed Since First COVID-19 Death | |
| Washington State (2018 pop. 7.5 million) | 1.11 | 21 |
| South Korea (2018 pop. 51.6 million) | 0.20 | 29 |
So what is to be done? For those on the medical front lines of the struggle and those directly supporting them the path is pretty clear. The rest of us need to support those folks and each other. Don't panic, don't hoard. Don't worry about getting sick but do take scientifically supported steps to help prevent it.
For those who are able to do so, physical distancing and staying home as much as possible is probably the most critical task now. If you're not concerned about your own well-being then think about the others you might expose if you do get sick or the health resources you might take up that could have been used by someone who had a heart attack or a child hit by a car.
See also: "A Few Thoughts on COVID-19 - Part II"
Labels: COVID-19, government, health, medicine, politics, science, statistics
Wednesday, March 11, 2020
Where the Bodies Are Buried
Freddie Glusman, owner of Piero's: Want me to tell you a story?
Eugene Jarecki, director-writer of The King: Please.
FG: Casino. They filmed it here [in Piero's]. True Story. I know where the bodies are buried, some of them anyway.
EJ: How come?
FG: Because I'm Jewish. I move in the right circles. I kiss the right ass.
Source: At about 1:29:50 in The King, Jarecki's documentary/op-ed on Elvis Presley and America.
Labels: crime, film & television, Jews






{kind=link}