Monday, June 28, 2021
Two COVID Tidbits
In late March of 2020 I wrote:
A 2016 report published by the National Academies repeatedly raised concerns about the SNS inventory and the logistics of distributing it in an emergency. The chair of the committee that prepared that report, Dr. Tara O'Toole, presciently told NPR in 2016:Almost a year to the day after I published that Health Affairs has published "US Public Health Neglected: Flat Or Declining Spending Left States Ill Equipped To Respond To COVID-19". The article is behind a pay wall so I haven't read it. The abstract says:
"We have drastically decreased the level of state public health resources in the last decade. We've lost 50,000 state and local health officials. That's a huge hit," says O'Toole, who wishes local officials would get more money for things like emergency drills. "The notion that this is all going to be top down, that the feds are in charge and the feds will deliver, is wrong."My point is that the inability and failure in the US to implement the successful model of South Korea to tamp down COVID-19 via widespread testing, contact tracing, and isolation of the exposed or infected was born of a longstanding failure of the values and priorities of the bipartisan political establishment and by the servile dependency and doltish complacency of the American people who keep electing them.
The COVID-19 pandemic has prompted concern about the integrity of the US public health infrastructure. Federal, state, and local governments spend $93 billion annually on public health in the US, but most of this spending is at the state level ... Although overall national health expenditures grew by 4.3 percent in this period, state governmental public health spending saw no statistically significant growth between 2008 and 2018 except in injury prevention. Moreover, state spending levels on public health were not restored after cuts experienced during the Great Recession ...
Axios reports: "The study found that public health spending dropped from $80.40 per capita in 2008 to $75.83 in 2018." It's worth pointing out that these figures understate the drop in public health spending. According to the U.S. Bureau of Labor Statistics CPI Inflation Calculator that $75.83 in June 2018 "has the same buying power as $65.85 in June 2008". Due to inflation, to maintain roughly the same per capita level as the 2008 public health spending would have required spending $92.59 per person in 2018.
###
... I consider it grotesquely unethical for government officials, vaccine manufacturers, and public health and medical professionals to conduct what is essentially a massive experiment* on hundreds of millions of people using relatively new vaccine technologies—mRNA and adenovirus vector vaccines—especially during a global pandemic. I am aware of no reason why Congress and health professionals couldn't and shouldn't have insisted that Operation Warp Speed funds be spent on conventional attenuated virus or viral protein vaccines.In a June 24, 2021, article titled "The mRNA Vaccines Are Extraordinary, but Novavax Is Even Better" Hilda Bastian reports in The Atlantic:
... the hype around the early-bird vaccines from Pfizer and Moderna has distorted perception. Their rapid arrival has been described in this magazine as "the triumph of mRNA"—a brand-new vaccine technology whose "potential stretches far beyond this pandemic."... It was easy to assume, based on all this reporting, that mRNA vaccines had already proved to be the most effective ones you could get—that they were better, sleeker, even cooler than any other vaccines could ever be.
But the fascination with the newest, shiniest options obscured some basic facts. These two particular mRNA vaccines may have been the first to get results from Phase 3 clinical trials, but that's because of superior trial management, not secret vaccine sauce. For now, they are harder and more expensive to manufacture and distribute than traditional types of vaccines, and their side effects are more common and more severe. The latest Novavax data confirm that it's possible to achieve the same efficacy against COVID-19 with a more familiar technology that more people may be inclined to trust.
Bastian continues:
... the success of the Novavax vaccine should be A1 news. The recent results confirm that it has roughly the same efficacy as the two authorized mRNA vaccines, with the added benefit of being based on an older, more familiar science ... Some of those people who have been wary of getting the mRNA vaccines may find Novavax more appealing.
The Novavax vaccine also has a substantially lower rate of side effects than the authorized mRNA vaccines ... Based on the results of Novavax's first efficacy trial in the U.K., side effects (including but not limited to fatigue) aren't just less frequent; they're milder too ... Side effects are a big barrier for COVID-vaccine acceptance.
Bastian concludes:
But here's what we know today, based on information that we have right now: Among several wonderful options, the more old-school vaccine from Novavax combines ease of manufacture with high efficacy and lower side effects. For the moment, it's the best COVID-19 vaccine we have.
Unfortunately, we don't have the Novavax vaccine yet and, as far as I know, Novavax hasn't applied to the FDA for emergency use authorization yet.
Labels: COVID-19, government, health, medicine, science, technology
Tuesday, May 11, 2021
The Safety of US COVID-19 Vaccines Revisited
After I finished my "The Safety of US COVID-19 Vaccines" post I learned that last week Tucker Carlson had done an episode on the same subject, including the use of VAERS data.
I don't typically agree with everything Carlson says and he is sometimes less careful than I think he should be. However, his segment on "How many Americans have died after taking the COVID vaccine?" is almost perfect. Don't trust me, watch it yourself.
What I want to focus on in this post is the outpouring of dishonest criticism from the rest of the mainstream media in the wake of Carlson's piece. In an all too typical example, rather than refute Carlson with relevant facts, National Review contributor Pradheep J. Shanker tweeted:
Tucker, being an idiot, took that number of deaths, and says they are related to the vaccine.
This, of course, is nonsense. But again, gullible people will believe these things, because the math and science isn’t exactly crystal clear.
In fact, Carlson simply and accurately reported what is in the VAERS data. Here's a representative passage:
... So the question is how do those numbers compare to the death rate from the coronavirus vaccines now being distributed across the country? That’s worth knowing.
We checked today. Here’s the answer, which comes from the same set of government numbers that we just listed: Between late December of 2020, and last month, a total of 3,362 people apparently died after getting the COVID vaccines in the United States. Three thousand, three hundred and sixty-two — that’s an average of 30 people every day. So, what does that add up to? By the way, that reporting period ended on April 23. We don’t have numbers past that, we’re not quite up to date. But we can assume that another 360 people have died in the 12 days since. That is a total of 3,722 deaths. Almost four thousand people died after getting the COVID vaccines. The actual number is almost certainly much higher than that — perhaps vastly higher.
The data we just cited come from the Vaccine Adverse Events Reporting System — VAERS — which is managed by the CDC and the FDA. [VAERS] has received a lot of criticism over the years, some of it founded. Some critics have argued for a long time that [VAERS] undercounts vaccine injuries. A report submitted to the Department of Health and Human Services in 2010 concluded that "fewer than one percent of vaccine adverse events are reported"* by the [VAERS] system. Fewer than one percent. So what is the real number of people who apparently have been killed or injured by the vaccine? Well, we don’t know that number. Nobody does, and we’re not going to speculate about it ...
The faux "fact checkers" at Politifact gave Carlson a rating of "false" on their "Truth-o-Meter". How did they justify their rating? Here a sample: "... VAERS data is considered unreliable for drawing causal conclusions. And dying after a vaccine is not the same thing as dying because of the vaccine."
I listened to the segment twice, Carlson did not draw a causal connection and never implied or claimed dying after a vaccine is the same thing as dying because of the vaccine. In short, Politifact's case against Carlson is a classic straw man argument—they thrash away at things Carlson didn't say.
Near the close of their article, Politifact says: "The CDC analyzed the VAERS death reports and concluded that there's no 'causal link to COVID-19 vaccines.' " I rate this claim mostly false. What the CDC actually says is: "A review of available clinical information, including death certificates, autopsy, and medical records has not established a causal link to COVID-19 vaccines" (emphasis in original).
The CDC did NOT say "there's no 'causal link to COVID-19 vaccines' ", as Politifact claims. They said a causal link had not been established but they also did not rule out a causal link. It's also worth noting that the CDC provides no further information about who conducted their "review" or how it was conducted. There's no link to any documentation of the review.
* The report Carlson reference is from 2011, here's more context from it:
Adverse events from drugs and vaccines are common, but underreported. Although 25% of ambulatory patients experience an adverse drug event, less than 0.3% of all adverse drug events and 1-13% of serious events are reported to the Food and Drug Administration (FDA). Likewise, fewer than 1% of vaccine adverse events are reported. Low reporting rates preclude or slow the identification of “problem” drugs and vaccines that endanger public health. New surveillance methods for drug and vaccine adverse effects are needed.
Labels: COVID-19, government, health, media, medicine, science, technology, Tucker Carlson
Sunday, May 09, 2021
The Safety of US COVID-19 Vaccines
People sometimes ask me if I've gotten a SARS-CoV-2 vaccine yet. My answer is always no. This usually prompts a query as to why I haven't been vaccinated.
My standard answer is that I'm not an anti-vaxxer, I get a flu shot every year. However, I add, I consider it grotesquely unethical for government officials, vaccine manufacturers, and public health and medical professionals to conduct what is essentially a massive experiment* on hundreds of millions of people using relatively new vaccine technologies—mRNA and adenovirus vector vaccines—especially during a global pandemic. I am aware of no reason why Congress and health professionals couldn't and shouldn't have insisted that Operation Warp Speed funds be spent on conventional attenuated virus or viral protein vaccines. That said, until today I usually added that I thought the new technologies would probably prove safe.
* As the FDA notes all of the COVID vaccines in use in the US today have been approved under as investigational drugs under an Emergency Use Authorization. The FDA Letter of Authorization for the Pfizer vaccine says: "Pfizer-BioNTech COVID‐19 Vaccine is for use for active immunization to prevent COVID-19 ... It is an investigational vaccine not licensed for any indication." Its "Investigational New Drug application (IND) number" is 19736. According to the FDA: "Emergency Use IND allows the FDA to authorize use of an experimental drug in an emergency situation ..."
Today, I actually looked at the CDC's and FDA's Vaccine Adverse Event Reporting System (VAERS) data for the first time. What I learned was pretty amazing.
As you can see from Table 1 below the number of deaths recorded as adverse events associated with COVID-19 vaccines is almost exactly the same as the number of death associated with all other vaccines since 2006 (all VAERS data reported in this post was selected by vaccination year).
| Table 1. (VAERS data as of May 10, 2021 for 2006-2021) | ||||
|---|---|---|---|---|
| Adverse Event Type | ||||
| Vaccine Type | Death | Life Threatening |
Permanent Disability |
Sum |
| COVID-19 | 3,729 | 3,362 | 2,379 | 9,470 |
| All Other Vaccines | 3,733 | 9,648 | 9,174 | 22,555 |
| Sum | 7,462 | 13,010 | 11,553 | 32,025 |
From 2016 through April 30, 2021, there were 4,621 deaths reported as adverse events associated with all vaccines in the US (there's no table in this post for that data).
Table 2 covers 2016-2021 and compares deaths associated with the COVID vaccines and the non-COVID vaccine (Prevnar 13) associated with the most deaths in the same time period. For comparison purposes I also added in the flu vaccine type associated with the most deaths.
As you can see there are far more deaths associated with COVID vaccines even though they have been in use for only a few months. An apples-to-apples comparison would require other data, including the number of doses of each vaccine administered in the selected time period. However, I could not find that data for the non-COVID vaccines although the CDC said that in the 2020-2021 flu season the estimated number of quadrivalent flu vaccines expected to be available was 195 million.
 |
| Table 2. (VAERS data as of May 9, 2021; click on images to enlarge) |
Table 3 gives the breakdown by COVID vaccine manufacturer of the following combined adverse events: Deaths, Life Threatening, and Permanent Disability. At first glance, it may look like the Janssen (Johnson & Johnson) vaccine is safer but as you can see from Table 4 far fewer doses of that vaccine have been administered.
 |
| Table 3. (VAERS data as of May 9, 2021) |
 | |
| Table 4. (CDC data as of May 9, 2021) |
Combining the data from Tables 3 and 4 we find that there were 11,209 doses (numbers are rounded) of the Janssen vaccine administered for every associated serious adverse event recorded in Table 3. The corresponding count for the Pfizer and Moderna vaccines are 33,951 and 28,423, respectively.
It's interesting to me that I have not read or heard any mainstream reporting on the relatively large, as compared to other vaccines, number of deaths associated with COVID vaccines as adverse events. There are four things to bear in mind about the current numbers: First, an adverse event report is not proof that the vaccine caused the adverse event; Second, the number of adverse events associated with COVID vaccines is tiny compared to the number of adverse events caused by the virus itself; Third, many adverse events including deaths go unreported for a variety of reasons**; and, Fourth, the reporting of adverse events associated with COVID vaccines is just getting started. Who knows how things will look in five or ten years? Hopefully, there will be no great increase adverse events associated with COVID vaccines that emerges long term. Time will tell.
** According to the CDC's VAERS summary page: "VAERS data are from a passive surveillance system. Such data are subject to limitations of under-reporting, reporting bias, and lack of incidence rates in unvaccinated comparison groups." This echoes findings in a workshop summary published in 1994 by the National Academies Press: "As a passive surveillance system, VAERS suffers problems of both underreporting and overreporting. Although health care professionals are required to report some adverse events, specifically, those that are covered by the no-fault component of the Vaccine Injury Compensation Program, there are no provisions for enforcement. It is likely that many events that occur after the receipt of vaccines, like those that occur after the receipt of medications, go unreported."
###
There is a March 31, 2021, letter in the medical journal, Circulation Research, titled "SARS-CoV-2 Spike Protein Impairs Endothelial Function via Downregulation of ACE 2" that some COVID and COVID vaccine deniers/skeptics are using innaccurately to scare people about COVID vaccines. For example, HEALTHRANGER says:
The prestigious Salk Institute, founded by vaccine pioneer Jonas Salk, has authored and published a bombshell scientific article revealing that the SARS-CoV-2 spike protein is what's actually causing vascular damage in covid patients and covid vaccine recipients, promoting the strokes, heart attacks, migraines, blood clots and other harmful reactions that have already killed thousands of Americans ... Critically, all four covid vaccine brands currently in widespread use either inject patients with the spike protein or, via mRNA technology, instruct the patient's own body to manufacture spike proteins and release them into their own blood. This floods the patient's body with the very spike protein that the Salk Institute has now identified as the smoking gun cause of vascular damage and related events (such as blood clots, which are killing many people who take the vaccines).However, in the very first paragraph of the Salk Institute news release it says:
LA JOLLA—Scientists have known for a while that SARS-CoV-2’s distinctive “spike” proteins help the virus infect its host by latching on to healthy cells. Now, a major new study shows that the virus spike proteins (which behave very differently than those safely encoded by vaccines) also play a key role in the disease itself.
The authors of the letter itself conclude with this: "... our results suggest that the S protein-exerted EC damage overrides the decreased virus infectivity. This conclusion suggests that vaccination-generated antibody and/or exogenous antibody against S protein not only protects the host from SARS-CoV-2 infectivity but also inhibits S protein-imposed endothelial injury" (emphasis added). There is a hyperlink to an article in the paragraph I quoted above from the Salk Institute that goes into greater detail on this subject. I recommend reading it.
###
In the final analysis one ought always to be skeptical of powerful people and institutions but also of their critics. My read of the data and science is that the new vaccine technology, not the spike protein, is probably more to blame for the comparatively higher rates of adverse events associated with COVID vaccines. I will be cautious going forward but as of now I plan to receive the Novavax vaccine—a more conventional viral protein vaccine type—when it becomes available.
Last revised: 11 May 2021
See also: "The Safety of US COVID-19 Vaccines Revisited"
Labels: COVID-19, government, health, media, medicine, science, technology
Wednesday, November 18, 2020
How Right-Wing Media Outlets Mislead on COVID-19
I complain about the routine dishonesty of mainstream and Left media outlets because they are my main sources of news and commentary. However, I have zero illusions about the routine accuracy and integrity of Right media outlets.
A case in point is a recent article by Jordan Davidson on the site of The Federalist titled: "Major Study Finds Masks Don't Reduce COVID-19 Infection Rates". In the body of Davidson's article it is claimed: "A high-quality, large-scale Danish study finds no evidence that wearing a face mask significantly minimizes people's risk of contracting COVID-19."
However, right in the Danish article's abstract the authors, Bundgaard et al., state: "Although the difference observed was not statistically significant, the 95% CIs are compatible with a 46% reduction to a 23% increase in infection."
Davidson writes:
After a month, 42 of the mask-wearers in the study (1.8 percent) were infected with the virus while 53 of the non-mask-wearers (2.1. percent) were infected with the virus. Statistically, this is not a significant difference between the two groups, suggesting these infection differences were a product of chance, say the study authors.
Echoing similar misinformation from the New York Times, Davidson again misleads her readers by misrepresenting the meaning and importance of a lack of statistical significance.* In fact, Bundgaard et al. use the word "chance" exactly nowhere in their article. They actually describe their findings as "inconclusive" rather than attributable to mere "chance".
In the "Discussion" section of the Bundgaard et al. article it says:
The findings ... should not be used to conclude that a recommendation for everyone to wear masks in the community would not be effective in reducing SARS-CoV-2 infections, because the trial did not test the role of masks in source control of SARS-CoV-2 infection. [emphasis added]
In other words, Davidson did exactly what the authors said she shouldn't do based on their work.
In the "Discussion" the authors again note that one of several limitations of their study was that it made "no assessment of whether masks could decrease disease transmission from mask wearers to others." In other words, the study offers no evidence about whether masks do or don't prevent COVID-19 infected mask wearers from infecting other people.
Moreover, as Bundgaard et al. indicate in their "Intervention" section, they were testing the effects of "no mask recommendation" versus "a recommendation to wear a mask". They were not testing masks or mask wearing per se. Also, only "46% of participants wore the mask as recommended" but Bundgaard et al. did not exclude from their results people in the mask recommendation group who were "predominantly" but not fully compliant with the mask recommendation. Only the 7% whose compliance was characterized as "not as recommended" were excluded.
In short, the Danish study says what pretty much any sensible person already realized—masks alone are not a silver bullet but there is evidence that they do help reduce the spread of COVID-19 from infected people to non-infected mask wearers.
Liar, manipulators, and incompetents working in the media depend upon the fact that most people will never question their reporting or never question it enough to do their own research. It also bears remembering that reporters and editors are also fallible humans—not every error or falsehood reported is deliberate. In any case, when it comes to important matters never blindly trust a media outlet (or a politician) to be accurate or honest.
###
* A note on "statistical significance": Davidson is not alone in botching the reporting on "statistical significance" the Danish authors do it, too. In 2019's, "Moving to a World Beyond 'p < 0.05' " the editors of the journal of the American Statistical Association write:
... it is time to stop using the term "statistically significant" entirely. Nor should variants such as "significantly different," "p < 0.05," and "nonsignificant" survive, whether expressed in words, by asterisks in a table, or in some other way.
Regardless of whether it was ever useful, a declaration of "statistical significance" has today become meaningless. Made broadly known by Fisher's use of the phrase (1925), Edgeworth's (1885) original intention for statistical significance was simply as a tool to indicate when a result warrants further scrutiny. But that idea has been irretrievably lost. Statistical significance was never meant to imply scientific importance, and the confusion of the two was decried soon after its widespread use (Boring 1919). Yet a full century later the confusion persists.
They also offer this guidance:
- Don't base your conclusions solely on whether an association or effect was found to be "statistically significant" (i.e., the p-value passed some arbitrary threshold such as p < 0.05).
- Don't believe that an association or effect exists just because it was statistically significant.
- Don't believe that an association or effect is absent just because it was not statistically significant.
- Don't believe that your p-value gives the probability that chance alone produced the observed association or effect or the probability that your test hypothesis is true.
- Don't conclude anything about scientific or practical importance based on statistical significance (or lack thereof).
Labels: COVID-19, critical thinking, health, media, science, statistics
Wednesday, November 04, 2020
Lessons of the 2020 Election
Donald J. Trump has endured more than four years of constant public drubbing by most of the mainstream media, academia, and the entertainment industry. Trump survived the bogus Russiagate conspiracy and a failed impeachment related to Biden family dealings in Ukraine. A significant number of establishment Republicans betrayed their party to publicly campaign for Biden. Biden has collected far more campaign money ($1,380.1 million vs. $863.6 million) than Trump.
In many ways Trump's presidency has been an incoherent mess marked by numerous self-inflicted wounds, including but not limited to, bad policies and inept policy implementation. Yet, despite all this and during the worst pandemic in 100 years and the worst economy in 90 years, Trump once again defied the pollsters and pundits to mount a strong challenge to the presidential nominee of Democratic Party. It looks like Republicans will hold the Senate and cut the Democratic majority in the House to single digits. Meanwhile, in solid blue California voters soundly rejected an attempt by political elites to remove an anti-discrimination clause from the state constitution.
This all begs the question: Will Democratic (or Republican) elites learn the right lessons from the 2016 and 2020 elections and resolve to work "to form a more perfect Union, establish Justice, insure domestic Tranquility, provide for the common defence, promote the general Welfare, and secure the Blessings of Liberty"? Nah.
See also:
- Anointing Biden & Election Irregularity Allegations I
- "Tucker Carlson: A Vote for President Trump Is a Vote Against America's Ruling Class" by Joey Pietro for The Western Journal
- "Ketman And The Left's Problem" by Rod Dreher for The American Conservative
Labels: Biden, COVID-19, media, politics, race, Russia, Trump, Tucker Carlson, voting
Monday, November 02, 2020
Comparison of Select COVID-19 Death Rates
| COVID-19 Deaths Per 1,000,000 Population | Median Age of Population | |
|---|---|---|
| Republic of China (Taiwan) (pop. 23.6 million) | 0.3 | 42.3 |
| S. Korea (pop. 51.8 million) | 9 | 43.2 |
| Japan (pop. 125.5 million) | 14 | 48.6 |
| Norway (pop. 5.5 million) | 52 | 39.5 |
| Germany (pop. 80.2 million) | 128 | 47.8 |
| W. Virginia (pop. 1.8 million) | 256 | 42.4 |
| Canada (pop. 37.7 million) | 270 | 41.8 |
| Washington State (pop. 7.6 million) | 313 | 37.6 |
| California (pop. 39.5 million) | 448 | 36.3 |
| France (pop. 67.8 million) | 573 | 41.7 |
| Italy (pop. 62.4 million) | 646 | 46.5 |
| United Kingdom (pop. 65.8 million) | 689 | 40.6 |
| United States (pop. 332.6 million) | 715 | 38.5 |
| Michigan (pop. 10.0 million) | 773 | 39.7 |
| San Marino (pop. 34,232) | 1,237 | 45.2 |
| New York (pop. 19.5 million) | 1,732 | 38.7 |
| New Jersey (pop. 8.9 million) | 1,856 | 39.8 |
| Unless otherwise specified population estimates are for July 2020 and, along with median pop. age, are from the CIA's World Factbook. Death rates and U.S. state populations are from Worldometer. Median age for U.S. states is from World Population Review. | ||
Labels: COVID-19, health, medicine, science, statistics
Sunday, November 01, 2020
Cuomo & COVID-19
Thanks to a fawning, largely uncritical media and a feckless, gullible public, Gov. Andrew Cuomo of New York was able to falsely position himself this year as the COVID-19 anti-Trump. In May, The Guardian published an op-ed titled "Andrew Cuomo is no hero. He's to blame for New York's coronavirus catastrophe". The authors noted:
Andrew Cuomo may be the most popular politician in the country. His approval ratings have hit all-time highs thanks to his Covid-19 response. Some Democrats have discussed him as a possible replacement for Joe Biden, due to Biden’s perceived weakness as a nominee. And there have even been some unfortunate tributes to Cuomo’s alleged sex appeal.
All of which is bizarre, because Cuomo should be one of the most loathed officials in America right now. ProPublica recently released a report outlining catastrophic missteps by Cuomo and the New York City mayor, Bill de Blasio, which probably resulted in many thousands of needless coronavirus cases ...
Federal failures played a role, of course, but this tragedy was absolutely due, in part, to decisions by the governor.
Nevertheless image triumphed once again over reality, as The Atlantic put it last August:
The opening night of the Democrats’ virtual convention was the beginning of a coronation for Joe Biden, but it was also a victory march for Andrew Cuomo, New York’s governor and a supposed hero of the coronavirus pandemic. “For all the pain and all the tears, our way worked,” Cuomo declared in his five-minute speech. “And it was beautiful.”
“Beautiful” is an odd way to describe a virus that has killed more than 25,000 New Yorkers, or about 15 percent of the total number of Americans who have died from COVID-19. But Cuomo has long been a curious leader for Democrats to hold up as an emblem of successful leadership during the pandemic: He has somehow presided over the worst and deadliest coronavirus outbreak in the country while eluding the widespread criticism that has surrounded both President Donald Trump and New York City’s Democratic mayor, Bill de Blasio.
Earlier today I had bizarre conversation about one of Cuomo's many failures. In 2015, the New York State Task Force on Life and the Law (TFLL), its members appointed by Cuomo, released its "2015 Ventilator Allocation Guidelines".
The TFLL estimated that during the "peak week" of a severe "1918-like" pandemic scenario the state would have a ventilator shortfall of 15,783 units (p. 30). Instead of urging the state's leaders to come up with a plan to close the shortfall of ventilators and trained personnel to operate them the TFLL accepted a shortage of life-saving equipment as a fait accompli. The TFLL was focused on rationing ventilators without any analysis of whether the shortage could be ameliorated through advance preparation. Cuomo implicitly, if not explicitly, agreed he could live with the projected shortage and the deaths that would entail.
Their solution, then, was to create a triage plan that, by design, likely consigned hundreds, if not thousands, of patients to a needless death when the pandemic arrived this year. When I pointed out this to my friend she defended Cuomo asserting there was little or nothing he could have done differently. I replied he could have said: This is unacceptable, we need to figure out how to close this gap. She claimed, "That's not how government works." I'll never understand why some people make excuses for corrupt and/or inept politicians.
In 1984, the governor's father, Mario Cuomo, who was then himself governor of New York, gave one of his best known speeches at the Democratic national convention. His vision of government included the idea that people should be "protected in those moments when they would not be able to protect themselves." Andrew Cuomo echoed this notion when, in 2017, he asserted of the subway "crisis": "There is no time for delay and there is no tolerance for a lack of
commitment on this issue ... The fundamental responsibility of government is to respond in a timely and effective way when people need help."
If Cuomo's TFLL could identify the problem then they could also have come up with a better solution. Moreover, Cuomo could have demanded one. No, he can't magically conjure ventilators or the money to buy them but experts have been predicting a serious viral pandemic for years. Cuomo (and governors and legislators across the country) had the ability and responsibility to ensure his state was better prepared for it.
Instead in March, Cuomo lied or betrayed a profound ignorance. As Colin Kalmbacher at Law & Crime wrote:
On Wednesday morning, during his quotidian Coronavirus press briefing, the three-term Democratic governor told an easily verifiable falsehood about New York’s state of health.
“No one has these ventilators and no one ever anticipated a situation where you would need this number of ventilators to deal with a public health emergency,” Cuomo said–explaining the Empire State’s recent move toward rationing the highly in-demand medical devices.
“So we have purchased everything that can be purchased,” he added. “We’re now in a situation where we’re trying to accelerate production of these ventilators, and a ventilator is a complicated piece of equipment.”
But Cuomo’s claim that “no one ever anticipated” the “number of ventilators to deal with a public health emergency” is directly undercut by a report from New York State itself–under his own administration–released halfway into Cuomo’s second term in office.
Like Cuomo, the New York State Commissioner of Health he appointed, Howard A. Zucker, was also given to uttering falsehoods. In a letter accompanying the TFLL's report he claimed: "Protecting the health and well-being of New Yorkers is a core objective of the Department of Health." So, Zucker knew about the anticipated ventilator shortage and the "death panel" solution to deal with it.
Yet, in March of this year, Newsday reported:
"I always felt if you can improve the life of others — whether an individual or many — you should," he [Zucker] said in an interview. "I learned practicing clinical medicine that I have to do everything possible ... it's our role in society."
"But I never expected this kind of situation," he said of the coronavirus threat."
Zucker has mostly flown under the radar compared to his boss but his COVID-19 performance prompted one editorial titled: "New York health chief Howard Zucker: Call him Dr. Death".
By April, Cuomo was throwing tens of millions of dollars around to try to buy ventilators at elevated prices from people who often couldn't deliver. If instead, he had ordered 15,783 ventilators in 2015 when his Task Force released its report then the state would likely have had a stockpile on hand during the COVID-19 crisis for less than 0.14% of the state's 2015-16 disbursements.
For the calculation above, I used a 2020 ventilator retail price via ProPublica of $12,495 per unit. I have no doubt that price is actually significantly higher than a competitive bidding process in 2015 would have obtained. If the state had spread the acquisition out over five years then the cost would have been less than 0.03% of the annual budget.
In any event, it seems both unsurprising and clear that few high-profile politicians of either major party actually concern themselves much with the victims of COVID-19, whom they largely regard as superannuated drags on the economy or otherwise disposable people. They don't say this out loud but their policies speak volumes. Instead of taking effective steps to save lives and safely re-open the economy, Democrats blame Trump, Republicans blame China (or engage in various forms of denial) and, in the meantime, the US has the largest COVID-19 death toll and one of the highest per capita COVID-19 death rates in the world.
Labels: Biden, COVID-19, Democrats, government, health, media, medicine, politics, science, Trump
Saturday, March 28, 2020
A Few Thoughts on COVID-19 - Part II
One week ago, I wrote:
As of today, the global COVID-19 fatality rate (deaths divided by aggregate confirmed infections) is about 4.1%.
We know that the actual fatality rate is probably significantly lower than 4.1% because not everyone who has been infected has been tested.
There are a lot of other factors leading to uncertainty over the actual fatality rate from COVID-19 that I didn't write about. There is an excellent discussion of the "Coronavirus (COVID-19) Mortality Rate" that elaborates on those factors. I recommend it.
Today, the crude global COVID-19 fatality is about 4.6% per figures from the UW Novel Coronavirus (COVID-19) Infection Map. I still have every expectation that the final rate will be much lower than 4.6% globally, in Italy, the US, and elsewhere. However, because of the failures mentioned in my earlier post I still fear that "the progression of the COVID-19 in the US will likely resemble Italy's trajectory more closely than South Korea's or China's." Nothing that's happened in the last week has dissuaded me from that view although I remain hopeful something will change.
A week ago, I also wrote: "By the end of next week we may start to see how effective efforts to flatten the curve have been in Washington state." The Governor of Washington believes this may be the case but in my reading of the data it's still too soon to know for sure.
I want to elaborate a bit on the comparison I made between the US and South Korea. China, in my opinion, is the wrong place to look for comparisons. Although China has some aspects of a market economy, large and important entities are state-owned enterprises directly controlled by the Communist Party of China (CPC) and the remaining sectors are subject to indirect CPC control in the one-party authoritarian regime.
There is evidence that the Chinese government suppressed key information about the virus at least in the early stages. In contrast, South Korea has a modern, mostly private market economy with a political system that is, by one measure, at least as democratic as the United States' "flawed democracy" (but see here for a different ranking).
One of the big mistakes that many people will undoubtedly make in the aftermath of COVID-19 is to demand a larger, more centralized public health and medical system in the US. One of the big pitfalls of such thinking is that centralization creates the risk of severe consequences from a single point of failure.
We are actually seeing that play out in the US where state and local public health agencies and officials take their lead from the federal government and were slow to react appropriately to the threat of COVID-19. They were also hamstrung by their dependence on the Centers for Disease Control and Prevention (CDC) to roll out COVID-19 testing and misplaced reliance on supplies from the Strategic National Stockpile (SNS).
One counterargument is, yes, but if the federal government had done its job correctly then we wouldn't be in this situation. True enough but there are no guarantees that when a crisis develops there will be an able, humane leader at the helm of the large, centralized ship of state.
I am aware of no compelling evidence that, say a President Hillary Clinton, would have prepared for or handled the COVID-19 crisis markedly better than Trump. Speculatively, we can say she may indeed have risen to the challenge of COVID-19 but Clinton would have been under the same pressures by the investor class not to disrupt their profit-taking and to win re-election this year.
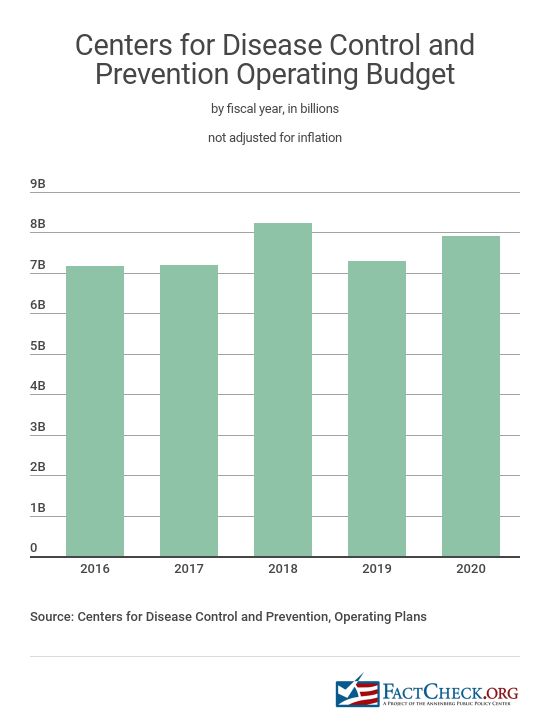
More crucially, the lapses in the CDC and the SNS, for instance, didn't develop under Trump alone. I have been unable to find a concise depiction of inflation-adjusted CDC annual budgets (there is this though) but it's clear that the Obama administration proposed significant cuts in 2011 (-11%). In 2013, the Obama administration again proposed more cuts in "biodefense and emergency preparedness programs" along with a $38 million reduction in the "allocation for the Strategic National Stockpile of emergency medical supplies".
And as NBC reports:
[The] U.S. strategic stockpile isn't intended to be the solution to a crisis. It's designed to be used as a stopgap during emergencies. The stockpile has limited resources, government officials and public health experts say, which weren't at full capacity even before the coronavirus was on the horizon.And:
The stockpile wasn't at full capacity before the COVID-19 outbreak in the U.S., in part because it never fully replenished some of the critical supplies used in the 2009 H1N1 pandemic response ...A 2016 report published by the National Academies repeatedly raised concerns about the SNS inventory and the logistics of distributing it in an emergency. The chair of the committee that prepared that report, Dr. Tara O'Toole, presciently told NPR in 2016:
"We have drastically decreased the level of state public health resources in the last decade. We've lost 50,000 state and local health officials. That's a huge hit," says O'Toole, who wishes local officials would get more money for things like emergency drills. "The notion that this is all going to be top down, that the feds are in charge and the feds will deliver, is wrong."My point is that the inability and failure in the US to implement the successful model of South Korea to tamp down COVID-19 via widespread testing, contact tracing, and isolation of the exposed or infected was born of a longstanding failure of the values and priorities of the bipartisan political establishment and by the servile dependency and doltish complacency of the American people who keep electing them. Trump surely deserves a lot of blame for his failures but much of the finger pointing by, for example, Michigan Gov. Whitmer, is simply not grounded in fact and is counter-productive, self-interested blame-shifting by culpable partisans in the midst of a major crisis.
It bears stating that governments weren't invented for the well-being of commoners and only servile fools would willingly depend upon them for that. Governments were created to secure and enhance the power of the already powerful and to provide rhetorical cover for that domination. That is not to say they cannot potentially be transformed by people to more closely reflect the rhetoric of, say, "life, liberty, and the pursuit of happiness" but we should never forget that decent treatment of ordinary people is, at best, a means, not an end, of government.
If we are to have a centralized state or any state at all then, ceteris paribus, one that could competently stop an COVID-19 epidemic, for instance, would be preferable but this is a false dichotomy. There are other, better ways for humans to organize themselves free from the coercive state if only we will imagine and create them.
See also: "A Few Thoughts on COVID-19"
Labels: anarchism, COVID-19, government, health, medicine, politics, science, Trump
Saturday, March 21, 2020
A Few Thoughts on COVID-19
Don't be deceived, COVID-19 is more lethal and more infectious than the normal annual influenza outbreaks. As one example, in roughly three weeks COVID-19 has already killed almost as many people in the Seattle area (King, Snohomish, and Pierce counties) alone as have died so far from the flu (lab-confirmed cases) in the entire State of Washington during the 2019-2020 flu season and COVID-19 shows no sign of slowing down yet. In part, this is because almost no one has any natural or vaccine-induced immunity to COVID-19 as it is "novel" and there is no vaccine for it.
Everywhere that COVID-19 has infected large numbers of people it has quickly overwhelmed the local health care system. That means the death toll from COVID-19 is added on to the existing, more routine causes of death from heart disease, cancer, influenza, accidents, etc. and the rapid influx of those sick from this new disease impairs the health care system's capacity to manage more typical cases of disease and trauma.
If unchecked by effective public health measures or natural immunity COVID-19 has exponential growth rates of infection and death (see also here and here and here) although the death curve is much flatter because the disease does not kill at nearly the same rate as it infects or sickens people. As of today, the global COVID-19 fatality rate (deaths divided by aggregate confirmed infections) is about 4.1%.
We know that the actual fatality rate is probably significantly lower than 4.1% because not everyone who has been infected has been tested. In South Korea, where there are high rates of testing and a very successful public health response, the fatality rate is about 1.2%. By contrast, the US 2018-2019 influenza fatality rate was about 0.1%. (There are a lot of factors, such as quality of the health care system, mean population age, smoking rates, etc., that influence fatality rates.)
Below, from the University of Washingon Novel Coronavirus (COVID-19) Infection Map, are two images (click to enlarge) showing the exponential growth of COVID-19 infections and deaths in the US and Italy.


The graphic below demonstrates that exponential growth of infection and death from COVID-19 can be arrested. South Korea had its first confirmed COVID-19 death on February 21 and in about three weeks it had stopped the initial exponential growth of infections. The number of COVID-19 deaths there is currently 102. China, too, after early missteps has reportedly stopped local transmission of COVID-19 altogether.

We did have earlier warnings to alert us to the potential of a dangerous viral pandemic. In addition to the Spanish Flu (1918; 25,000,000 - 100,000,000 deaths), there was the Asian flu (1957; 1,000,000 - 2,000,000 deaths), Hong Kong flu (1968; 1,000,000 - 4,000,000 deaths), SARS-CoV (2002; 774 deaths), H1N1 flu (2009; 151,000 - 575,000 deaths), and MERS-CoV (2012; 862 - 912 deaths). MERS is notable because it has a high fatality rate (~37%) and continues to infect and kill people every year. With few exceptions, the media, public health community, and politicians of all political stripes failed to alert Americans to the very real dangers of a viral pandemic and the country is, thus, woefully unprepared.
Unfortunately, I am afraid the progression of the COVID-19 in the US will likely resemble Italy's trajectory more closely than South Korea's or China's. I hope I will be proven mistaken in this.
American individualism is, in many ways, pathological and more communal attitudes and behavior are not necessarily antithetical to freedom or a healthy individualism. Whatever their downside, a more community-oriented culture was one factor that evidently contributed to the successful Chinese and South Korean responses to COVID-19.
If competently led, adequately staffed, and sufficiently provisioned, I think America's decentralized health care system could have responded in a coordinated and effective manner. This was not the case, however, and one result has been the very slow roll out of widespread COVID-19 testing that would have enabled the early isolation of infected people. The US also has a warped, hollowed out industrial base that has left it dependent on the importation of key health care supplies—masks, drugs, reagents, gloves, ventilators, etc.—that were seemingly not stockpiled and/or aren't being distributed in sufficient quantities.
Chinese health officials were able to successfully confine the COVID-19 outbreak to primarily one region of the country and then bring the resources of the rest of the country to bear in order to tamp down the disease. Unfortunately, for reasons described above, the US has failed to keep the outbreak of disease concentrated in one or two regions.
The result is that the COVID-19 is now, apparently, spreading exponentially in every US state. The first US death from COVID-19 was on February 29, 2020. Since that time Washington has had 82 more deaths, New York 43, California 24, Louisiana and Georgia 14 each, New Jersey 11, and Florida 10. COVID-19 deaths have been reported in several other states, too. The wide geographic dispersion of infections in the US will likely make it immensely difficult to bring COVID-19 under control quickly. Again, I hope I am proven wrong in this.
By the end of next week we may start to see how effective efforts to flatten the curve have been in Washington state. However, even if they have been effective the state has already fallen far short in comparison to South Korea. Consider the table below based on the 2018 populations.
| COVID-19 Deaths Per 100,000 Population | Days Elapsed Since First COVID-19 Death | |
| Washington State (2018 pop. 7.5 million) | 1.11 | 21 |
| South Korea (2018 pop. 51.6 million) | 0.20 | 29 |
So what is to be done? For those on the medical front lines of the struggle and those directly supporting them the path is pretty clear. The rest of us need to support those folks and each other. Don't panic, don't hoard. Don't worry about getting sick but do take scientifically supported steps to help prevent it.
For those who are able to do so, physical distancing and staying home as much as possible is probably the most critical task now. If you're not concerned about your own well-being then think about the others you might expose if you do get sick or the health resources you might take up that could have been used by someone who had a heart attack or a child hit by a car.
See also: "A Few Thoughts on COVID-19 - Part II"
Labels: COVID-19, government, health, medicine, politics, science, statistics






{kind=link}